
Psychiatric Support for OCD
Psychiatric care for OCD is a structured treatment plan consisting of diagnosis, medication management, and therapy coordination provided by a psychiatrist.
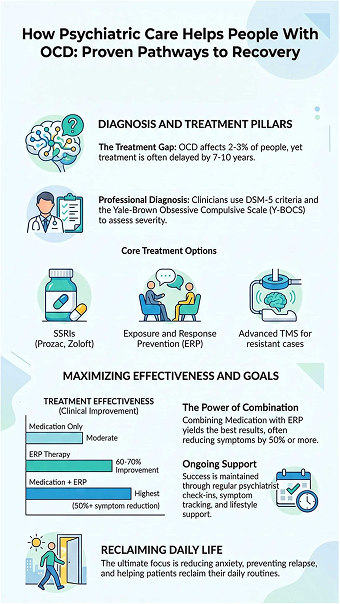
They then check in to see what’s working and what isn’t, making changes along the way. About 2 to 3 percent of people have OCD. On average, individuals with OCD delay treatment by 7–10 years after symptom onset.
OCD is defined by two core components: obsessions (intrusive thoughts) and compulsions (repetitive behaviors performed to reduce anxiety). Without treatment, this cycle takes over. The aim of support is straightforward, to help people reclaim control of their daily life. Keep reading to see how this support works in real life.
Key Takeaways
- Treatment usually includes diagnosis, medication, and therapy, which can reduce symptoms by nearly half for many people.
- Exposure and Response Prevention is a proven therapy that helps about two-thirds of people in structured programs.
- If standard treatments are not effective, options like Transcranial Magnetic Stimulation, an FDA-cleared method, may be considered.
How Do Psychiatrists Diagnose OCD Accurately?
A key diagnostic attribute is time consumption, with symptoms typically exceeding one hour per day or causing significant functional impairment. If you’re losing over an hour a day to rituals, the label matters less than the immediate need for a strategy to take that hour back. While I follow the DSM-5 criteria, with symptoms typically exceeding 1 hour per day or causing significant functional impairment.
If you’re losing over an hour a day to rituals, the label matters less than the immediate need for a strategy to take that hour back.
The official rulebook is the DSM-5. It says a diagnosis needs obsessions, compulsions, or both. But the real key is how much room these thoughts and actions take up. If they eat more than an hour of your day, or if the struggle to manage them is crushing, that’s a major signal. The goal is to see how much of your life has been handed over to rituals and fear.
As noted by National Institutes of Health (NIH)
“Obsessive-Compulsive Disorder (OCD) is a prevalent psychiatric disorder affecting 1% to 3% of the global population, characterized by intrusive thoughts, known as obsessions, and repetitive actions, or compulsions. These symptoms affect patients not only by consuming a significant portion of their time but also by causing marked distress and functional impairment” – StatPearls
So how do they find this out? Psychiatrists conduct repeated, structured interviews across multiple sessions to ensure diagnostic consistency. These aren’t quick chats; they’re detailed interviews that pick apart your thoughts and routines.
They’ll ask the same questions in different ways, sometimes over several visits, to get a consistent picture. When I administer the Yale-Brown Obsessive Compulsive Scale (Y-BOCS),The Yale-Brown Obsessive Compulsive Scale (Y-BOCS) evaluates symptom severity, resistance, and control over compulsions.
As a clinician, seeing a patient attempt to fight a compulsion, even if they fail, is a massive indicator of how they will respond to ERP therapy. It’s an objective measure used by the world’s leading specialists to predict treatment paths.
It’s surprisingly easy to get this wrong. People can spend five, even ten years being treated for something else. OCD symptoms often get tangled up with depression, general anxiety, or tic disorders. In fact, most people with OCD have at least one other condition. That overlap is why diagnosis can be messy.
To figure things out, doctors gather a few important clues.
They start with a long, detailed interview. It covers your personal history, your thoughts, and your daily habits. This conversation goes deep. It looks at the specifics of how you live.
Then, they usually turn to a standard tool. One common example is the Y-BOCS scale. This isn’t about passing or failing. It measures the severity of symptoms. It looks at how much time they consume. It checks the level of distress they create. The resulting score paints a clearer picture of the overall effect.
A single clue isn’t enough. I complete the diagnostic story by merging your personal history with the Y-BOCS score. This combination reveals the full impact of OCD on your life. That’s how they build a reliable diagnosis.
In my years of practice, I’ve seen that getting this right is less about a checklist and more about unmasking a ‘chameleon.’ I often look for the ‘hidden rituals’, the mental compulsions like silent praying or counting, that patients don’t realize are part of the disorder. A truly original diagnosis looks at the intent behind the thought, not just the thought itself.
What Role Does Medication Play in OCD Treatment?

When doctors treat OCD, they often begin with SSRIs. These are drugs like Prozac (fluoxetine) or Zoloft (sertraline). They work by increasing serotonin in the brain, which helps lower anxiety and the power of intrusive thoughts.
Getting results takes time, usually 8 to 12 weeks. The doses needed for OCD are often higher than for depression. Finding the right dose is a careful balancing act. You need enough to help, but you also have to watch for side effects. For 40 to 60% of people, this leads to a real reduction in symptoms. The goal isn’t to erase thoughts, but to turn down the anxiety so therapy can actually work. Psychiatric Evaluations in Raleigh can help determine whether medication is the right starting point for your situation.
As highlighted by Mayo Clinic
“The FDA has approved three TMS devices , BrainsWay, MagVenture and NeuroStar , to treat OCD in adults. These devices are used when traditional treatment hasn’t been effective.” – Mayo Clinic
What if SSRIs don’t work?
There are other paths to try. The options include:
- Clomipramine: An older, strong antidepressant that often works well for OCD, but it can have more side effects.
- Antipsychotic Augmentation: Adding a very low dose of a drug like risperidone to an SSRI for a stronger effect.
- TMS (Transcranial Magnetic Stimulation): A non-surgical treatment using magnetic pulses to target overactive brain circuits. It’s like a gentle reboot for stuck pathways.
Medication doesn’t fix OCD by itself. Its real job is to lower the distress enough for a person to do the hard work in therapy. For many, that combination is what finally makes a difference.
Why Is Exposure and Response Prevention (ERP) the Gold Standard?
ERP is the most effective therapy for OCD. It breaks the disorder’s core cycle.
An obsessive thought causes panic. The compulsion, like washing or checking, feels like the only way to stop it. This gives short-term relief but reinforces the fear long-term. ERP interrupts this pattern.
Therapy feels like a controlled, guided challenge. We start with easier triggers to build confidence, proving anxiety fades on its own if you don’t perform the ritual.
How it works in practice
The steps are direct:
- Expose yourself to a trigger.
- Prevent the usual compulsive response.
- Repeat until the anxiety decreases naturally.
This isn’t just talking. It’s active, experiential learning that rewires the brain’s reactions. About 60-70% of people who complete ERP see significant, lasting improvement.
When compared to other options, the difference is clear:
| Treatment Type | Effectiveness | Long-Term Benefit |
| ERP Therapy | High (60–70%) | Strong |
| Medication Only | Moderate | Medium |
| ERP + Medication | Highest | Strongest |
This last point is key. For many, medication and ERP are a powerful team. An SSRI can lower the overall level of anxiety, making it possible to even start the challenging work of ERP. Together, they offer the best chance for lasting change by both calming the nervous system and teaching it new rules.
How Do Psychiatrists Combine Medication and Therapy?

Think of treating OCD like managing a chronic illness. You don’t just take a pill and hope for the best. You need a coordinated strategy, and that’s where a psychiatrist’s skill comes in.
The most common approach pairs medication with a specific type of therapy called Exposure and Response Prevention (ERP), which is central to how OCD Treatment in Raleigh NC They have different jobs. Medication, usually an SSRI, works in the background to dial down the general volume of anxiety. This doesn’t cure the obsessions, but it makes them less deafening.
That lower volume is what makes ERP possible. ERP is the hard, active work of facing fears without performing compulsions. High baseline anxiety levels reduce ERP adherence, making pharmacological stabilization clinically beneficial. Medication can help bring that starting point down to a 6 or 7.
A psychiatrist’s role is to manage this balance in real time. They don’t just write a prescription and send you to therapy. They monitor your side effects, adjust doses based on how therapy is going, and stay in contact with your therapist.
If you’re hitting a wall in ERP sessions, they might tweak your medication to give you a bit more stability. If the medication causes fatigue that interferes with therapy, they’ll look at other options. It’s a constant, active adjustment.
The data backs this up. Using medication and ERP together is about 25-30% more effective than using either one alone. The practical benefits are straightforward:
- Therapy feels less like torture and more like tough, but manageable, work.
- Symptoms tend to improve faster.
- You’re less likely to slide back after making progress.
When this first-line combination isn’t enough, psychiatrists can layer in other tools, like adding a low-dose antipsychotic or referring for TMS. But even these advanced options are almost always used with ongoing therapy, not as a replacement for it.
The goal is always the same: use medication to create a window of opportunity, and use therapy to teach you how to live differently on the other side of that window.
What Ongoing Support Do Psychiatrists Provide?
OCD requires ongoing management due to its chronic and relapsing nature; it’s more like getting a map for a long trip. The path isn’t straight, and sometimes you hit rough patches. A psychiatrist’s job is to be your guide for the whole journey, not just the first mile.
The core of ongoing support is regular check-ins. These aren’t just quick chats to refill a prescription. They’re structured appointments where you review what’s How Psychiatrist Help With Mental Health working and what isn’t.
You’ll talk about your symptoms, any side effects from medication, and how therapy is going, often starting with a psychiatric evaluation in Raleigh.
The psychiatrist uses these visits to spot small warning signs, like a compulsion starting to creep back in, and make tiny adjustments to your plan. This proactive approach can stop a minor slip from becoming a major relapse.
A huge part of this is managing the overlap with other conditions. It’s very common for someone with OCD to also struggle with depression or another anxiety disorder. Treating just the OCD while ignoring a deepening depression usually backfires. A psychiatrist works to treat the whole picture, adjusting strategies so progress in one area doesn’t come at the expense of another.
So what does this long-term support actually look like? It’s a mix of practical steps:
- Fine-tuning medication: Finding the right dose is an ongoing process. As life changes, your needs might too.
- Symptom tracking: Using simple scales or a journal to objectively see patterns, rather than relying on memory.
- Psychoeducation: Explaining why OCD happens demystifies it. Knowing it’s a faulty brain signal, not a character flaw, reduces shame.
- Lifestyle coordination: Talking about sleep, diet, and stress management. These don’t cure OCD, but letting them fall apart makes everything harder.
This consistent, steady presence changes the relationship with the illness. Instead of frantically seeking help during a crisis, you develop a maintenance routine. You learn to recognize your own early warning signs and have a trusted professional to contact. The goal shifts from just surviving episodes to building a stable life where OCD is managed, not in charge.
Why Do Some OCD Treatments Fail or Feel Ineffective?
Approximately 30–40% of patients show partial or delayed response to first-line OCD treatments. Several factors explain why.
Misdiagnosis is one issue. OCD can resemble other anxiety disorders. If the diagnosis is off, treatment targets the wrong problem.
ERP effectiveness depends on protocol adherence, including proper exposure intensity and avoidance of reassurance behaviors. ERP must be done correctly. If therapists offer too much reassurance, the process weakens. The goal is to face anxiety without relying on safety behaviors. When that step is skipped, progress slows.
Medication can be another barrier. OCD often requires higher doses than other conditions. Side effects such as fatigue or emotional dullness can lead patients to stop taking them.
Other common challenges include:
- Late diagnosis, which allows habits to become deeply fixed
- Burnout from long treatment periods
- Limited access to specialists trained in OCD care
These setbacks do not mean treatment has failed. They often signal the need for adjustment. With the right changes, many patients regain progress.
How Does Psychiatric Care Improve Quality of Life in OCD?

Effective OCD treatment improves functional outcomes, including task completion time, social engagement, and occupational performance treatment does more than reduce symptoms. It changes how people move through their day.
As symptoms ease, routines become less interrupted. Tasks that once took hours can be completed without repeated checking or rituals. This shift affects work, school, and relationships.
Many patients report:
- Fewer compulsions interrupting daily tasks
- Better control over anxiety
- Improved focus and confidence
Even a 50 percent reduction in symptoms can make a clear difference. Symptom reduction leads to improved daily routine stability and reduced decision-making delays. Decisions feel easier. Relationships carry less tension.
For those who do not respond to standard care, options like transcranial magnetic stimulation may offer another path. These treatments target brain activity linked to OCD and can support other methods.
How Does Psychiatric Help People With OCD Long-Term?
OCD is typically a chronic condition requiring long-term symptom management rather than full remission. It requires long-term care, built on consistency rather than quick fixes.
Psychiatrists help patients maintain progress through ongoing treatment plans. These often include medication, therapy such as ERP, and regular check-ins. The goal is to keep symptoms manageable and prevent relapse.
Starting treatment early improves outcomes. When OCD patterns go untreated for years, they become harder to change. Early support limits that buildup.
Long-term care focuses on:
- Keeping symptoms stable over time
- Adjusting treatment as life changes
- Preventing relapse through regular follow-up
For difficult cases, additional tools like transcranial magnetic stimulation may be added. These options expand what treatment can offer, especially when standard methods are not enough.
OCD does not vanish overnight. Symptom improvement typically occurs gradually over months of consistent treatment adherence, through steady care and small gains. With the right support, people can reduce symptoms and regain control over their daily lives.
Finding Steady Ground with OCD Care
You know how exhausting it feels when your thoughts won’t slow down and every small decision turns into a loop you can’t escape. It wears you out. The right care brings structure back, helping you regain control step by step through therapy and steady support that actually fits your life.
If you’re ready for a clearer path forward, support like Medpsychnc can make things feel more manageable without adding more stress. TMS offers a non-invasive, FDA-cleared option for patients with treatment-resistant OCD. You can start by learning more or reaching out to Medpsychnc and take that first step toward relief.
FAQ
How does Cognitive Therapy differ from Cognitive Behavioral Therapy for OCD?
Cognitive Therapy focuses on changing negative thought patterns linked to intrusive thoughts.
Cognitive Behavioral Therapy combines this with behavioral therapy to address compulsive behaviors. Psychiatrists often use both approaches together for better results. This combined method improves cognitive control and reduces the obsessive-compulsive cycle.
Can Acceptance and Commitment Therapy help with OCD symptoms?
Acceptance and Commitment Therapy helps patients accept intrusive thoughts without reacting to them. It focuses on mindfulness meditation and values-based actions instead of avoidance. This approach supports stress reduction and builds healthier behavioral patterns. Psychiatrists may include it as part of a broader treatment plan.
What role do group therapy sessions play in OCD treatment?
Group therapy sessions provide a support community for people with Obsessive Compulsive Disorder. Patients share experiences and learn coping strategies in a structured setting. This approach also improves mental health awareness and reduces isolation. Psychiatrists may combine it with individual therapy for better outcomes.
How do imaginal exposure and in vivo exposure help OCD treatment?
Imaginal exposure involves mentally facing feared situations in a controlled way. In vivo exposure uses real-life exposure therapy to confront triggers directly. Both methods are part of exposure and response prevention therapy. They help reduce anxiety and weaken compulsive behaviors over time.
Can Habit Reversal Therapy be used for OCD-related behaviors?
Habit Reversal Therapy helps patients become aware of repetitive behavioral patterns. It teaches alternative responses to replace compulsive or ritualistic behavior. This method is useful for conditions like Excoriation Disorder linked to OCD. Psychiatrists may include it in a structured behavioral therapy plan.
References
- https://www.ncbi.nlm.nih.gov/books/NBK553162/
- https://www.mayoclinic.org/diseases-conditions/obsessive-compulsive-disorder/diagnosis-treatment/drc-20354438?srch_tag=qzfmntiz7veqces6punnmrvzzugj7ubj&p=1



